
Why not offer your patients the benefits of PD?
PD and kidney transplant
A kidney transplant is the goal for many end-stage renal disease (ESRD) patients but may not always be an option at the start of their renal replacement therapy.
Patients treated with PD before kidney transplantation had improved patient survival and similar graft survival compared with those treated with in-center HD.8
Empower your patients’ independence through PD1–4
Dialysis therapy is a long journey. PD allows your patients the freedom to stay at home longer.
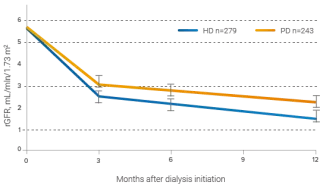
After adjustment for baseline variables and dropout, averaged over time, PD patients averaged 30% higher rGFR than HD patients over a 12-month period (p<.0001)10
Therapeutic benefits of preserving RRF are numerous
- Fluid removal11
- Sodium removal11,12
- Phosphate removal11,12
- Middle molecule clearance11,12
- Erythropoietin production11
- Reduced left ventricular hypertrophy11,12
- Survival benefit11
Why preserving residual renal function is key
Residual Renal Function (RRF) is better preserved in patients treated with PD compared to those treated with HD:10
- PD patients averaged a 30% (SE 8%) higher rGFR than HD patients (p<.0001) over a 12-month period.10
- PD patients experienced a slower rate of rGFR decline than HD patients.10
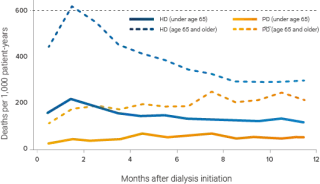
Preservation of RRF is associated with patient survival13
- Each 250 mL increase in daily urine volume was associated with a 36% lower relative risk of death.14
- A residual GFR increase of 1 mL/min/1.73 m2 resulted in a 12% reduction in relative risk of death.15

References
-
Kutner NG, Zhang R, Barnhart H, et al. Health status and quality of life reported by incident patients after 1 year on haemodialysis or peritoneal dialysis. Nephrol Dial Transplant. 2005;20(10):2159-2167.
-
Frimat L, Durand PY, Loos-Ayav C, et al. Impact of first dialysis modality on outcome of patients contraindicated for kidney transplant. Perit Dial Int. 2006;26(2):231-239.
-
Molsted S, Prescott L, Heaf J, et al. Assessment and clinical aspects of health-related quality of life in dialysis patients and patients with chronic kidney disease. Nephron Clin Pract. 2007;106(1):c24-c33.
-
Rubin HR, Fink NE, Plantinga LC, et al. Patient ratings of dialysis care with peritoneal dialysis vs. hemodialysis. JAMA. 2004;91(6):697-703.
-
North American Pediatric Renal Trials and Collaborative Studies. NAPRTCS 2011 Annual Dialysis Report. Available at: https://web.emmes.com/study/ped/annlrept/annualrept2011.pdf.
-
Kutner NG, Zhang R, Huang Y, et al. Depressed mood, usual activity level, and continued employment after starting dialysis. Clin J Am Soc Nephrol. 2010;5(11):2040-2045.
-
Bodin S, editor. Contemporary Nephrology Nursing. 3rd ed. Pitman, NJ: Janetti Publications Inc.; 2017. p.154, 221-222.
-
Molnar MZ, Mehrotra R, Duong U, et al. Dialysis modality and outcomes in kidney transplant recipients. Clin J Am Soc Nephrol. 2012;7(2):332-341.
-
United States Renal Data System. 2016 USRDS Annual Data Report: Vol. 2 – ESRD in the United States. Ch. 6:395-396.
-
Jansen MA, Hart AA, Korevaar JC, et al. Predictors of the rate of decline of residual renal function in incident dialysis patients. Kidney Int. 2002;62(3):1046-1053.
-
Wang AYM, Lai KN. The importance of residual renal function in dialysis patients. Kidney Int. 2006;69(10):1726-1732.
-
Perl J, Bargman JM. The importance of residual kidney function for patients on dialysis: a critical review. Am J Kidney Dis. 2009;53(6):1068-1081.
-
National Kidney Foundation. 2006 Updates Clinical Practice Guidelines and Recommendations. Guideline 3:57.
-
Bargman JM, Thorpe KE, Churchill DN. Relative contribution of residual renal function and peritoneal clearance to adequacy of dialysis: a reanalysis of the CANUSA study. J Am Soc Nephrol. 2001;12(10):2158-2162.
-
Termorshuizen F, Korevaar JC, Dekker FW, et al. The relative importance of residual renal function compared with peritoneal clearance for patient survival and quality of life: an analysis of the Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD)-2. Am J Kidney Dis. 2003;41(6):1293-1302.
-
Mendelssohn DC, Mujais SK, Soroka SD, et al. A prospective evaluation of renal replacement therapy modality eligibility. Nephrol Dial Transplant. 2009;24(2):555-561.
-
Oliver MJ, Garg AX, Blake PG, et al. Impact of contraindications, barriers to self-care and support on incident peritoneal dialysis utilization. Nephrol Dial Transplant. 2010;25(8):2737-2744.
-
Han SH, Lee SC, Ahn SV, et al. Improving outcome of CAPD: twenty-five years’ experience in a single Korean center. Perit Dial Int. 2007;27(4):432-440.