
Incremental PD
Incremental PD
Starting dialysis at less than full dose when there is still significant renal function1
Person-centered approach
Incremental PD decreases workload of dialysis2
Multiple Benefits
Incremental PD may preserve kidney function better than full dose dialysis3
Start with Incremental PD and preserve the choice of PD
Physician to her patient: Physician Survey
Outcomes
Incremental PD strategies achieve outcomes that are at least as good as full dose PD prescriptions in patients with RKF1
RKF
RKF preservation without increased risk of peritonitis3,5,*,†
Hospitalization Rates
Lower hospitalization rates vs. standard PD5,†
Protection of Patient Modality
Protection of patient modality goal6
• PD option often lost at low GFR if insufficient time for catheter insertion and training
• Urgent start PD often not available
Benefits
Benefits may include7,8
• Improvement of uremic symptoms
• Reduces burden on patient
• Allows more time for the patient to adjust to dialysis therapy
• Minimized glucose exposure
Cost
Lower cost9
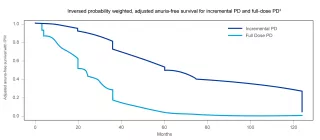
Incremental PD was beneficial for preserving residual renal function as demonstrated by a longer anuric free time as compared to full-dose PD.3
Overall median time to the first peritonitis was 2.3 years for patients on Incremental PD and full dose3,*
Study Design
A single center, retrospective cohort study of incident patients (n=347 patients between January 2007 through December 2015) was conducted to compare incremental PD with full-dose PD with the following specifications3
* Study design: A retrospective, randomized study (n=347 patients) between 2007-2015, comparing patients on incremental PD and full dose PD. Primary outcome in the study was anuria-free survival comparing IPD and full dose PD. Inversed probability weighted, adjusted anuria-free survival using time-dependent Cox proportional hazards model. This was an observational, single-center study, which included only CAPD patients with >200mL daily urine volume.
† Study design: A 10-year single center study (n=100) between 2002-2012 comparing incident patients on incremental PD and standard PD.
Previous page
PD allows patients to dialyze at home and minimize the risk of viral infections
Next page
Prioritize PD, a more cost-effective therapy than ICHD, to lower overall healthcare costs and, with Remote Patient Management (RPM), to reduce hospitalization costs
References
-
Baxter Data on File, IPD market research October 30,2019.